Case Study: A Guide to Using the TRACE Framework
PART 1
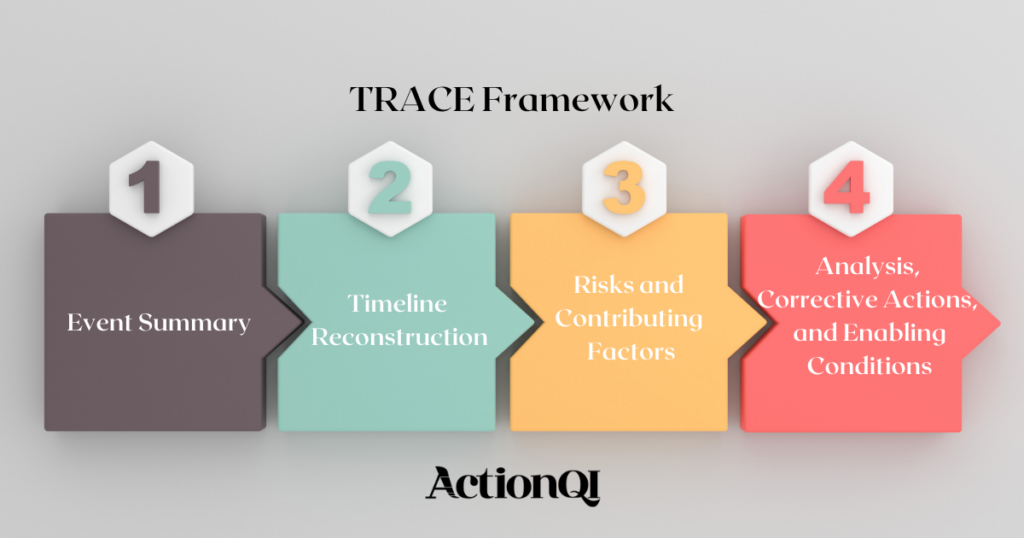
This case study was developed as a practical walkthrough of the TRACE Framework. The goal of this exercise is to practice structured investigation using incomplete and non-linear information, build skill in identifying relevant signals across clinical and operational data, and strengthen your ability to reconstruct events, risks, and contributing conditions without being led to conclusions.
Before you begin, download the TRACE Framework Template. Read the case below in full first, then use the guide to complete each section of the TRACE framework.
The Case
The patient arrived from a step-down unit late in the evening after a prolonged stay complicated by respiratory decline and intermittent hypotension requiring vasopressor support. A central line had been placed several days earlier during a period when the ICU was managing multiple admissions from the emergency department surge, with bed turnover occurring faster than usual. Nursing documentation from earlier shifts notes that the dressing was reinforced once due to loosening edges after repeated patient repositioning during imaging transport, though no full dressing change was documented at that time.
Over the next several days, intake and output records show fluctuating fluid balance with periods where charting lagged behind real-time care activities during high-acuity interventions. The patient intermittently received parenteral nutrition, which was paused and restarted depending on gastrointestinal tolerance. A note from pharmacy reflects a delay in TPN compounding one afternoon due to a supply shortage of lipid emulsion, requiring substitution approval and staggered delivery.
Family members were frequently present and asked questions about line use, especially after observing multiple staff accessing the same lumen during a brief episode of desaturation. One visitor reportedly mentioned concern that “the line looked touched a lot,” though this was not escalated in real time. During a shift change, bedside report was shortened due to an incoming trauma activation, and handoff documentation was partially completed after staff were reassigned.
On one morning, the patient developed a low-grade fever that was initially attributed to possible atelectasis, given recent reduced mobility and intermittent refusal of incentive spirometry. A respiratory therapist later documented inconsistent participation in pulmonary exercises, noting the patient was “tired and less engaged than prior days.” Blood cultures were drawn later than ordered due to competing priorities during a unit-wide catheter insertion procedure happening simultaneously in another room.
Environmental services documented a delayed terminal clean in an adjacent room, leading to temporary storage of supplies in a shared alcove near the patient’s doorway. Some supply carts were observed being used across multiple rooms during a staffing shortage on the night shift, when two nurses called out unexpectedly and float staff were reassigned from another specialty area. A traveling nurse unfamiliar with local central line maintenance protocols documented uncertainty about the standard scrub time for hub access but proceeded based on prior facility experience.
Two days after the initial fever, laboratory results returned showing elevated inflammatory markers, and the patient required escalation of vasopressor support. A note from infectious disease consultation references concern for bloodstream infection after blood cultures returned positive for a gram-negative organism. Around the same time, documentation shows the central line dressing was noted to be “clean, dry, and intact,” although a later photo review revealed slight lifting at one corner that had not been formally documented in the chart.
A brief quality review later questioned whether a chlorhexidine sensitivity might have contributed to localized skin irritation around the insertion site, as mild erythema had been noted earlier and attributed to adhesive reaction. No rash was documented elsewhere, and no alternative skin prep was trialed during the line’s maintenance period.
PART 2
TRACE Framework Reviewer’s Guide
- Event Summary
Begin by reviewing the case in full before attempting to summarize what occurred. Focus on building a clear, structured overview without interpretation or conclusions.
Coaching Questions
HAI Type
- What type of healthcare-associated infection is being investigated?
• Where in the care environment did device exposure or risk appear most relevant?
Organism
- What information is provided about the pathogen or organism?
• What limitations exist in what is known at this stage?
Patient Factors
- What aspects of the patient’s clinical condition may influence susceptibility or complexity of care?
• What therapies or conditions may increase exposure to infection risk?
Device Information
- What device(s) are involved in the patient’s care?
• What details are available about insertion timing, maintenance, or handling?
Outcome
- What clinical deterioration or escalation is described?
• What signals indicate possible infection progression?
Reflection Questions
- What information feels essential versus contextual background?
• What additional details would improve clarity of the situation?
Summary Event Findings
- Central venous catheter present for several days in ICU setting
• Intermittent vasopressor support and parenteral nutrition exposure
• Fever followed by hemodynamic deterioration
• Blood cultures positive for gram-negative organism
• Dressing integrity concerns noted later in review
Example
The case describes a patient with a central venous catheter in place during a prolonged critical illness complicated by hemodynamic instability. The patient later developed fever and clinical deterioration with blood cultures positive for a gram-negative organism, raising concern for a central line-associated bloodstream infection during the hospitalization period.
- Timeline Reconstruction
Begin by identifying key events without assuming order. Focus on how care conditions changed over time and how operational pressures may have influenced workflow.
Coaching Questions
- What are the earliest device-related events described?
• When do changes in patient condition first appear?
• What operational pressures are present during different phases of care?
• Where are there interruptions, delays, or documentation gaps?
• How do staffing or workload changes align with clinical events?
Reflection Prompt
Where do conditions of care delivery appear to shift in ways that could influence risk exposure?
Suggested Timeline (only after thinking space)
- Central line placed during period of high ICU surge and rapid bed turnover
• Dressing reinforcement documented after patient transport and repositioning episodes
• Intermittent TPN exposure with pauses due to tolerance and supply delays
• Staffing shortages and reassignment of float/travel staff in unit
• Family concerns raised about frequency of line access
• Shortened handoff during shift change due to trauma activation
• Fever onset following period of reduced mobility and intermittent respiratory therapy participation
• Delayed blood culture collection due to competing procedural priorities
• Environmental services delay leads to supply storage near patient area
• Infection markers rise and vasopressor escalation required
• Blood cultures positive for gram-negative organism
• Later review identifies dressing edge lifting not fully documented
- Risks and Contributing Factors
- a) System Factors
Coaching Questions
- How did staffing levels and workload influence care delivery?
• What operational pressures affected consistency of processes?
• Where were system interruptions or competing priorities evident?
Possible Findings
- ICU surge conditions with rapid admissions and turnover
• Staffing shortages due to call-outs and float reassignment
• Competing procedural demands delaying specimen collection
• Environmental constraints including delayed room turnover and supply storage in shared areas
- b) Knowledge
Coaching Questions
- Were there differences in practice approaches among staff?
• Was there uncertainty or variability in protocol use?
Possible Findings
- Traveling nurse uncertainty about standard scrub time for hub access
• Variation in central line maintenance approach based on prior facility experience
- c) Attitudes
Coaching Questions
- How did urgency or workload influence prioritization of tasks?
• Were any concerns deferred or not escalated?
Possible Findings
- Family concern about frequent line access not escalated in real time
• Competing priorities leading to delayed blood culture collection
- d) Beliefs
Coaching Questions
- What assumptions may have influenced interpretation of early signs?
• Were symptoms attributed to alternative explanations?
Possible Findings
- Fever initially attributed to atelectasis
• Mild erythema attributed to adhesive reaction
- e) Practices
Coaching Questions
- Were standard procedures consistently followed?
• Where were deviations or incomplete processes observed?
Possible Findings
- Dressing reinforcement without full documented change
• Shortened handoff process with incomplete documentation
• Supply carts used across multiple rooms during staffing shortage
• Unclear consistency in hub access scrub technique
4a. Analysis
Coaching Questions
- How do staffing, workload, and environment interact in this case?
• Where do delays compound over time?
• How might fragmented communication affect device maintenance reliability?
• How do competing priorities influence infection prevention practices?
Model Analysis
This case reflects multiple interacting pressures that shaped the reliability of central line care over time. High patient volume and ICU surge conditions created an environment where staff were managing frequent admissions, rapid bed turnover, and competing procedural demands. These conditions contributed to interruptions in routine workflows such as dressing maintenance, documentation, and timely specimen collection.
Staffing instability, including call-outs and reliance on float and traveling staff, introduced variability in practice approaches and reduced consistency in central line maintenance techniques. This variability is reflected in uncertainty about scrub times and reliance on prior facility experience rather than standardized local protocols.
Communication disruptions, including shortened handoffs and incomplete documentation during shift changes, limited continuity of situational awareness across teams. These gaps occurred alongside periods of high acuity events, where attention was diverted to urgent clinical priorities.
Environmental and logistical constraints, including delayed room turnover and temporary supply storage in shared spaces, increased operational complexity and may have contributed to increased line access frequency and variability in sterile handling conditions.
Over time, these overlapping pressures aligned with early subtle clinical signals that were initially attributed to alternative explanations, delaying escalation and reinforcing a pattern of fragmented recognition across shifts.
4b. Corrective Actions
Coaching Questions
- How could workflow reliability be strengthened under surge conditions?
• What system changes reduce variability in line maintenance practices?
• How can communication be improved during high-acuity transitions?
• What structural safeguards reduce reliance on individual discretion?
Model Corrective Actions
- Standardize central line maintenance protocols with visual aids at point of care
• Implement structured handoff tools that cannot be bypassed during surge events
• Introduce real-time documentation prompts for dressing changes and line access
• Create escalation pathways for patient or family concerns regarding device handling
• Reduce supply contamination risk by eliminating shared alcove storage near patient care areas
• Establish competency verification for traveling and float staff prior to independent line care
4c. Enabling Conditions
Coaching Questions
- What leadership support is required for sustained improvement?
• What staffing model adjustments would stabilize workflows?
• What monitoring systems could detect early variation in line care practices?
• What barriers might affect long-term adherence?
Model Enabling Conditions
- Stable staffing ratios aligned with acuity and surge capacity planning
• Leadership reinforcement of standardized device care practices across all staff types
• Continuous audit and feedback system for central line maintenance compliance
• Integration of documentation prompts into electronic health record workflow
• Environmental redesign to prevent cross-room supply sharing
• Ongoing onboarding and competency validation for temporary and rotating staff
TRACE Summary
- Most Significant Risks Identified
- Variability in central line maintenance practices
• Staffing instability and workload surges
• Fragmented communication during transitions
• Environmental and supply chain disruptions
- How Risks Accumulated Over Time
- Initial device placement during surge conditions created baseline variability
• Maintenance inconsistencies emerged with workflow interruptions and staffing changes
• Communication gaps and delayed escalation reduced early recognition
• Operational strain compounded across successive shifts
- Major Risk Themes
- Workflow fragmentation under high demand
• Inconsistent adherence to standardized device protocols
• Communication breakdown during transitions of care
• Environmental and logistical constraints affecting sterile practice
- Highest-Priority Improvement Opportunities
- Standardization of central line care processes
• Strengthening handoff reliability
• Reducing variability introduced by temporary staffing
• Improving environmental controls around supply handling
- Critical Enabling Conditions
- Stable staffing and surge planning infrastructure
• Integrated documentation and decision support tools
• Strong leadership reinforcement of standardized practices
• Continuous monitoring and feedback systems for device care reliability